COMPLAINTS GUIDANCE FAQ'S
Before making a complaint, please read the following section which discusses common concerns.
Frequently Asked Questions:
I have been told by a health professional that the frenulotomy performed on my baby was incomplete
It is advisable to speak directly with the health professional or service who undertook the procedure for a follow up conversation or appointment. It is impossible for someone who was not present at the time of the procedure to tell if there is reattachment or incomplete release. It is important for you and the practitioner to have that discussion and reassess the function of your baby’s tongue.
My baby’s tongue-tie has reattached / regrown and I wasn’t told to do stretches or disruptive wound management
Some babies have a restrictive frenulum once healing has taken place and this may require a further division. This restriction may be scar tissue that may need a month or more to settle. There is no published evidence that suggests disruptive wound management or stretches will prevent reattachment. It is thought that around 2-4%[1]of babies who have a tongue tie division will go on to have a second procedure and this seems to be the same whether or not disruptive wound management is used.
Disruptive would management is a controversial and emotive subject and the majority of practitioners in the UK don’t advocate it due to the lack of evidence and concerns about the risk of oral aversion and infection.
([1] From ATP audit and leaflet from a practice that is known to recommend disruptive wound management).
I wasn’t told to do any exercises to encourage my baby to mobilise their tongue following tongue-tie release.
Some practitioners suggest doing exercises that encourage movement, such as poking the tongue out. These are usually well tolerated and are non-invasive, however there is no research that proves they are effective.
My baby’s tongue-tie was missed by a tongue-tie practitioner
A frenulum is a normal structure that we all have, and it can be difficult to determine at what point it becomes a restrictive frenulum. Part of the assessment process should involve a feeding assessment, the use of tongue-tie assessment tools and the practitioner’s own experience to make a decision whether they think your baby’s frenulum is causing a problem with feeding. It’s also important to remember that in healthcare there are often differing opinions and a practitioner should make a reasonable judgement and be able to explain their reasoning for this to you.
Additionally, babies go through a lot of postural changes during pregnancy and birth. This can have an impact on a baby’s head, neck and jaw. This means that as a baby develops, over days and weeks, restrictions may become more evident.
The tongue-tie practitioner didn’t perform a frenulotomy – I want my money back.
It is reasonable for health professionals to charge a fee for their professional opinion, assessment and feeding support. Many practitioners will have a pricing structure that outlines cost of assessment and feeding support only with an additional cost for frenulotomy.
My baby has a tongue tie and although they don’t have feeding problems, I want to have it divided to prevent future issues
It is not considered good medical practice to undertake a procedure with some associated risks where there are no discernible benefits. So, if there are no symptoms experienced, a division may not be needed apart from in the most exceptional circumstances. Many people grow into adulthood with a restrictive frenulum but are able to adjust and adapt.
There is currently no direct correlation between tongue-tie and speech and language issues. It is advised to go back to your practitioner if feeding related problems develop.
My baby’s tongue-tie was divided incorrectly, or my baby has sustained injuries.
Your tongue-tie practitioner should have discussed the potential risk of injury with you when you were consenting to the procedure. All surgery comes with a small risk of unintended injury. If you believe the damage or injuries were as a result of negligence or malpractice, please refer to the complaints process below.
My baby’s tongue tie was divided but it hasn’t changed anything / there is no improvement
The suck, swallow, breathe pattern of a baby is complex. It can take several weeks for a baby to settle into a new pattern. Sucking exercises can help improve the muscle strength in the tongue which may have a low tone as a result of the restrictive frenulum. It can take several weeks for your baby to get used to the new mobility.
There can also be co-existing problems such as intolerances or muscular tensions in the head, neck and jaw. Some of the symptoms of tongue-tie overlap with these conditions. Do contact your practitioner for further support and if they are unable to help ask for a referral to someone who can support you further.
There is a chance that the procedure may not make a difference as your practitioner will have explained to you.
The tongue tie practitioner I saw did not provide any breastfeeding support during the consultation.
Whilst we believe it is good practice, we acknowledge that not all tongue-tie practitioners provide breastfeeding support. If breastfeeding support was offered as part of the consultation, please contact your practitioner in the first instance and if the response is not satisfactory please follow the flow chart below.
I have been told by my Midwife, Paediatrician, BF peer supporter etc – that my baby has a tongue tie and the practitioner I have contacted still wants to charge me for a full assessment rather than just for the procedure.
It is important that the person undertaking the procedure is satisfied that a frenulotomy is actually needed prior to undertaking a surgical procedure themselves. The assessment is required because the practitioner has full accountability for their practice.
The tongue tie practitioner I saw ‘missed’ my baby’s lip tie.
The Association of Tongue-tie practitioners has a position statement regarding lip-tie which can be found here
The tongue tie practitioner I saw did not suggest bodywork (e.g. osteopathy) for my baby.
Not all babies undergoing tongue-tie division will need to see a bodyworker. In certain situations, bodywork can be a useful intervention, but it is not a routine recommendation.
I am bottle feeding my baby and the tongue-tie practitioner will not divide for this reason.
The ATP supports tongue-tie release for any baby who is experiencing feeding difficulties as a result of a restrictive frenulum no matter the feeding method. Some NHS services are commissioned for breastfeeding babies only – but not all.
I didn’t feel safe because my practitioner wasn’t wearing personal protective equipment (PPE)
Strict infection control procedures should be in place at all times with additional measures during the COVID19 pandemic (such as wearing a face mask). Concerns such as these are serious, and the ATP would suggest following the complaints advice below.
I was not briefed about the risks and benefits of the procedure before the procedure was undertaken
For consent to be valid, it must be voluntary and informed, and the person making the decision must have the capacity to do so. The consent for tongue-tie release should be written consent. Consent can be withdrawn at any time. If you were not briefed about the risks and benefits of the procedure before it was undertaken, please do follow the complaints process outlined below.
I have received no follow up.
For practitioners to check that all is well and understand the outcomes of the procedure, some follow up is needed. This may be via telephone, email, text message or in person and may be undertaken by the person who undertook the procedure or by the referring infant feeding service. If you have received no follow up do contact the practitioner or service provider in the first instance because there could be an error in communication.
I have been unable to contact the service provider / practitioner following tongue-tie procedure
If you are using an NHS service and you are unable to contact them via telephone, email or text please do contact the Trust’s Patient Advice and Liaison Service (PALS) team.
Many private practitioners are solo workers and so they may not respond immediately. It is reasonable to expect some response with 72hrs of contact for existing clients, even if to acknowledge your attempts. If this is not satisfactory follow the complaints process below.
What can I do if a practitioner is not a member of the ATP?
You can still follow the complaints process below, but the ATP mediation service will not be available.
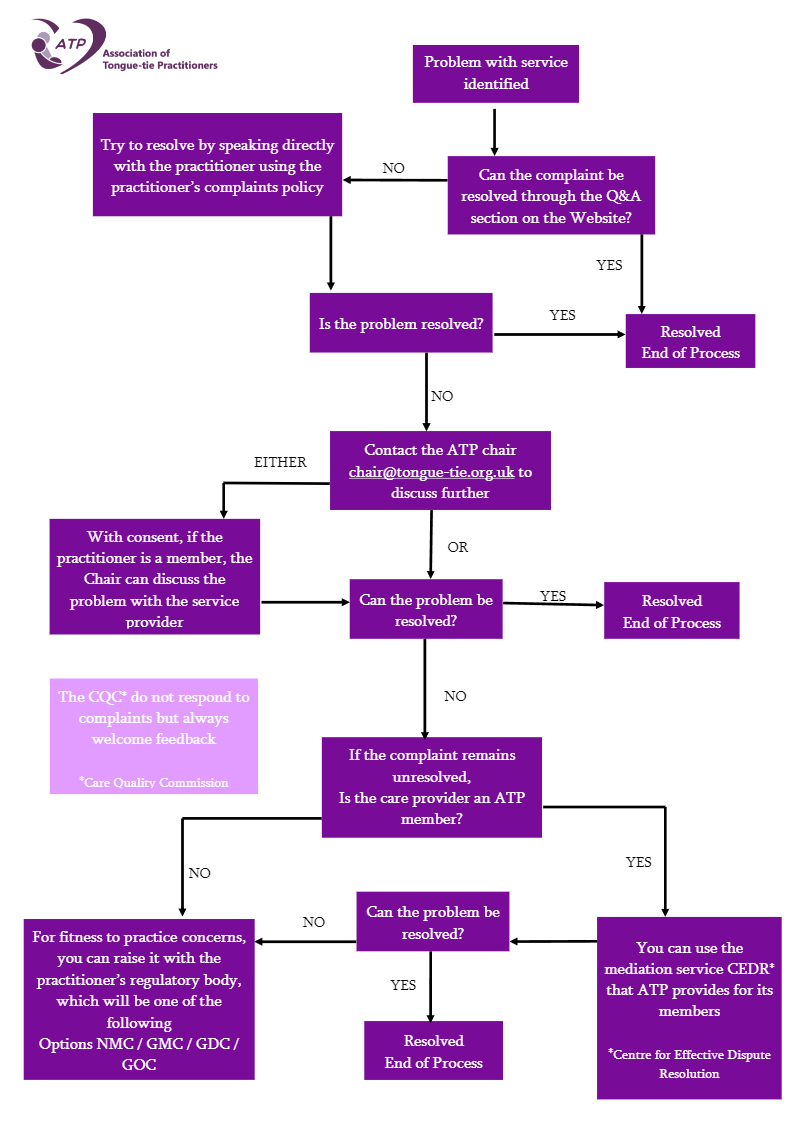
How to make a complaint regarding tongue-tie services:
In the first instance please read the frequently asked questions above.
Any complaint you wish to make should be put in writing to the service provider. If this is an NHS service, there will be a complaints department, or you can contact Patient Advice and Liaison Service (PALS). If you had private treatment the complaint should go direct to the individual or the service used.
A mediation service is available to all ATP members who are private practitioners that can be used if you are not satisfied with the outcome following your complaint.
If you have serious safety concerns about a practitioner your complaint can be escalated to their professional body such as the Nursing and Midwifery Council (NMC), the General Medical Council (GMC), the General Dental Council (GDC) or the General Osteopathic Council. This may result in a lengthy investigation into the individual’s fitness to practice.
You might also consider providing feedback to the Care Quality Commission (CQC). The CQC accepts feedback to help protect others from going through the same experience.